EMQ » July–September 2023 » Volume 59 Issue 4
[mepr-show rules=”100329″] [/mepr-show]
Summary: IHS Global developed a training process that equips healthcare workers around the globe to be witnesses for Jesus in their healthcare settings. The course combines curriculum (translated into global heart languages), training (in-person, virtual, or hybrid), and follow-up led by trained leaders who have a heart for equipping others and for sharing Christ.
By Latha Mathew and Lindsey Miller
As healthcare workers, we meet hurting people every day in healthcare settings. We hear about diseases, pain, loss of dear ones, war, and poverty. People look to us for answers far beyond the chief complaints they present. And this should be expected because disease is more than physical.
But how do we respond? As followers of Christ in healthcare, we can begin by asking: Is God at work? The answer is always, yes! It is in the context of a broken world that God calls us as Christians to be salt and light, caring for our patient’s spiritual needs in addition to their physical needs.
Many healthcare workers desire to be the expressions of God’s love to their patients, but they do not know how to start or are too busy to use the opportunity. Yet, what would the world look like if Christian healthcare workers were trained to make use of those precious moments with their patients for Jesus? What if they knew how to be witnesses for Jesus?
The Saline Process(ihsglobal.org/SalineProcess) is a training developed by IHS Global that equips healthcare workers around the globe to be witnesses for Jesus in their healthcare settings. The course combines curriculum (translated into global heart languages), training (in-person, virtual, or hybrid), and follow-up led by trained leaders who have a heart for equipping others and for sharing Christ.
Faith and Healthcare
Today’s scientific data shows that faith makes a difference in health outcomes.[i] It demonstrates that patients are open to spirituality and want their healthcare workers to talk to them about spiritual matters.[ii] It also reveals that best practices require an appropriate integration of faith and health.[iii] Studies also show that religion/spirituality helped patients in coping with illness and pain, diseases, and end-of-life issues.[iv] Patients with religious struggle had an increase in 2-year mortality rate compared to control patients.[v][vi]
During the early part of the COVID-19 pandemic, Google searches for “prayer” in 107 countries increased 30% (the highest ever recorded).[vii] Faith and health are connected. Therefore, religion and spirituality should not be missed by healthcare providers.
Beyond the scientific data, for those of us who are called to be Jesus’ disciples, the Bible reminds us of our calling to be witnesses of Jesus. In Matthew 5:13–16, Jesus tells us we are salt and light: salt that preserves lives and light that reflects the truth and reality of Jesus.
The saturation of salt that preserves lives is 0.9%. This is the normal saline we use in medical practice. It integrates sodium chloride and water. In the appropriate proportions, it is an essential lifegiving solution. Yet any variation in the concentration or its chemical identity and this solution no longer brings the desired healing to patients.
We are called to be life-giving spiritual saline to our patients and colleagues by integrating truth and love, always keeping in mind our identity as children of God. Approaching every patient with holistic care is not only excellent and ethical healthcare practice, but it is obeying God’s call.
Jesus perfectly lives out this integration as he helped people who came to him for healing by going beyond physical needs to address their emotional and spiritual needs. For example, Jesus’s healing of the woman who experienced bleeding for 12 years and the paralytic who was brought to Jesus through the roof both ended with Jesus emphasizing the spiritual aspect of their needs.
The Saline Process
Consider the woman at the well from John 4. Was she a professional disciple or evangelist? No. She was simply someone who met Jesus personally and couldn’t help but invite others to meet him, too. The Samaritan woman ran to the town and said to people, “Come, see …. Could this be the Messiah?” (John 4:29).
And many Samaritans came out to meet Jesus which led to them later saying to the woman, “We no longer believe just because of what you said; now we have heard for ourselves, and we know that this man really is the Savior of the world” (John 4:42). The woman at the well is the model for being witnesses that the Saline Process teaches.
Jesus explained the Samaritan’s process toward following him by saying, “Even now the one who reaps draws a wage and harvests a crop for eternal life, so that the sower and the reaper may be glad together. Thus, the saying ‘One sows, and another reaps’ is true. I sent you to reap what you have not worked for. Others have done the hard work, and you have reaped the benefits of their labor” (John 4:36–38). What happened with the Samaritan woman and the Samaritan community is what the Saline Process is all about.
Jesus talks about the work of cultivating and sowing as essential parts of the process to harvest (and even the harder part). We all have an opportunity to be a part of God’s work and each step of the process matters in the Kingdom work – cultivating, sowing, and harvesting – so we “may be glad together.”
A person coming to Jesus is a journey and not an event. It may take weeks, months or even years. In our healthcare setting we may not see many people accepting the Lord (the harvesting phase) but cultivating and sowing are equally important. We are called to do this hard work – to be life-giving spiritual saline – but we are not called to do it alone.
The Holy Spirit guides people’s lives and takes them on this journey to Jesus. We only have to stay tuned to the Holy Spirit and obey his prompting, walking with each person one step closer to Jesus. It is important to remember that each of us has different roles at different moments with the person we’re interacting with depending on his or her place in their faith journey. When one reads through the gospels, it becomes clear that Jesus did not use only one strategy for ministering to people. His stories, parables, teaching, actions, being, and more helped people understand, so we also can use different ways to reach people.
Recognizing a Great Opportunity
When we see past the hard work of our jobs, we realize that we have a privileged position, as health professionals, to share the love and reality of Christ. Often, we feel under pressure and without enough time. However, if we stop for a minute, we can see great opportunity. Francis Grim of Healthcare Christian Fellowship International (HCFI) said, “More people walk through the doors of the hospitals than through the doors of churches.”[viii]
There are an estimated 7.5 million Christian healthcare workers[ix] around the globe. With an average of 7,000 patient contacts per year per healthcare worker,[x] these witnesses have over 50 billion interactions for Christ annually. God has given Christian healthcare workers a great opportunity and a privileged position to meet patients at their time of need. We must consider this great responsibility.
A doctor attended a virtual Saline Process Witness Training course in November 2021. He described the training as useful, simple, practical, and also an opportunity for spiritual growth. He was able to put his training to work immediately.
His pastor called to tell him about a new couple in their church whose 3-year-old daughter was very sick. “I had just returned from a tiring day at work, but I thought this must be an opportunity that God was giving me to show His love,” he explained.
He went with a friend to see the family. The child was sobbing, while the parents tried to comfort her. When the doctor examined the little girl, he realized she had an acute condition of the abdomen and needed immediate medical assistance.
The family was poor, new to the area, and didn’t know anyone. The doctor and his friend prayed for God’s guidance. He decided to call a friend at the hospital. “… she said that she was the person on call for the pediatric surgery unit that evening. What a providence!”
The little girl received immediately attention. The doctor stayed with the parents while the staff at the hospital took the little girl in for surgery for intestinal obstruction. The doctor shared about the family with a few of his friends, and several responded by providing food, money, and blood donations. Many others also visited the family and prayed with them. The little girl recovered well, was discharged, and was taken home by her joyful parents.
God had provided the right kind of help at the right time, and the parents recognized this. God strengthened their faith. And because of their testimony, a cousin of theirs came closer to God and started attending church regularly.
“I thank God for giving me this opportunity to be a blessing to this family,” shared the doctor. “It was the Saline Process training that helped me to be sensitive to the Holy Spirit and seize the opportunity when it came.”
Being Aware of Barriers
This amazing opportunity available to healthcare workers is often not recognized or utilized adequately. This occurs because of a variety of barriers. For healthcare workers, these might include work pressures, time demands, inadequate knowledge, pride, fear, laziness, or even anxiety about negative attitudes from colleagues. These keep us from being life-giving saline to our patients. We miss out on the chance to treat the whole person. We remain focused on the physical needs without recognizing the emotional and spiritual needs of our patients.
Our patients also have barriers. Theirs may be fear, pain, misinformation, cultural differences, suspicions of people in authority, etc. These can keep them from hearing us when we share. The Saline Process looks specifically at emotional, intellectual, and volitional barriers in our patients, which all of these other barriers can fit within.
Each phase of the agricultural model – cultivating, sowing, and harvesting – corresponds with overcoming the three spiritual barriers: emotional, intellectual, and volitional. A good understanding of these barriers will help us diagnose where our patients are on their faith journeys in order to overcome barriers.
Emotional barriers can be overcome by cultivating or our loving presence with them. Intellectual barriers can be overcome by sowing or presenting truth. And volitional barriers can be overcome by harvesting or praying for a decision and having meaningful discussion with them. Throughout the process, healthcare workers continue to be the light that reflects Christ through their lives.
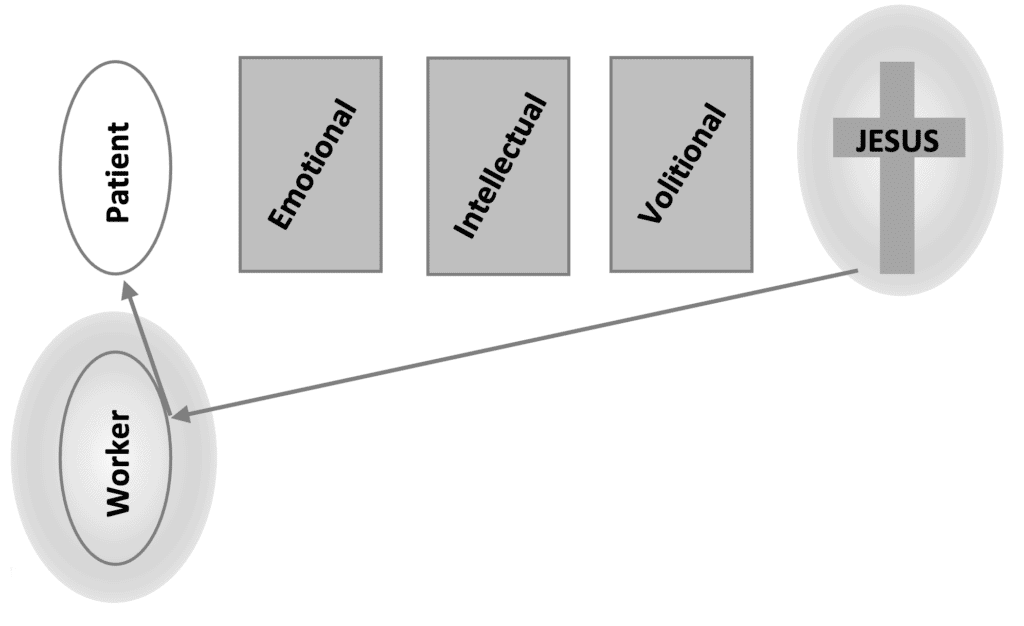
Caption: Figure 8.1 – Barriers to pointing people to Jesus.
Being vs Doing
What does it look like to be salt, light, and a witness for Jesus?
“But you will receive power when the Holy Spirit comes on you; and you will be my witnesses in Jerusalem, and in all Judea and Samaria, and to the ends of the earth” (Acts 1:8).
Jesus instructed us that we will be his witnesses. Jesus didn’t say, “Go witness.” He said, You will be my witnesses. This identity piece is at the core of engaging with others with Christ. In the same way, his saying, You are the salt and you are the light, conveys that we are his witnesses.
Being a witness for Jesus cannot be separated from being closely connected with Jesus and being transformed into his likeness. Spiritual vitality is the secret of the powerful life of biblical characters such as David, Daniel, Apostle Paul, as well as other role-models of faith who lived before us. Spending time with Jesus, helps us overcome barriers in our lives, and gain confidence and courage to be his witnesses. As our lives start to reflect the life of Christ, his love overflows from within us.
When our behaviors and attitudes reflect Jesus, our lives point our patients and our colleagues to Christ. The fragrance of a Christ-like character attracts people to us. They trust us when they observe our professional competence. They are comforted when they feel our compassion. Our wise communication can bring healing to them. These traits can be developed in us as we prayerfully and intentionally work with the Holy Spirit.
God will give us the courage to be his witnesses with humility and boldness. We can start right where we work now with the patients who sit in front of us. One first step could be to make our workplaces safe environments for patients instead of places of fear.
Tools for Cultivating, Sowing, and Harvesting
The Holy Spirit provides tools for cultivating, sowing, and harvesting. The first tool is prayer. We must prayerfully acknowledge the journey to Christ is God’s work and not ours, and then cover every moment from cultivating to harvesting in prayer. While we pray for our patients and colleagues to know Christ, we also need to ask others to pray that we will be effective witnesses for Jesus.
A tool for cultivating the heart is asking questions. These can help us develop understanding beyond medical issues. Questions can build relationships and trust. When healthcare workers ask patients, or even their colleagues, questions related to their family, job, or even their struggles, they can feel seen and validated. It can be healing.
We can take also take a spiritual history, much like medical history, to understand each patient’s spiritual background and current spiritual condition. This helps us to understand where they are on their spiritual journey. Taking a spiritual history is considered a best practice by many influential healthcare institutions today.[xi]
Faith flags are a tool for sowing biblical truth These are short statements that naturally let someone know you are a child of God without creating more barriers. These could be talking about how we found hope in God when we were in difficult situations that are similar to the patients. Faith stories can take patients that show interest further in depth. These can be sharing an experience about our own faith, but, again, in natural conversation.
Truth prescriptions invite someone who is receptive to faith to do, read, or watch something to help them grow towards faith in Christ. When a person is ready for harvest, a clear and easily understood presentation of the gospel is a logical next tool to use. We might do that through our own personal testimony.
Throughout the process, we might need the help of a spiritual referral team, much like we use a medical referral team in medical practice. This team can provide guidance or even be the next people on the journey.
Understanding this faith journey as a process can help us engage more meaningfully. We can then approach each patient with permission, sensitivity, and respect(1 Peter 3:15) out of love for our patient and the Lord. This helps us be more effective participants in Christ’s transforming work in each patient encounter.
Participating in God’s Kingdom Work
Ultimately, both our lives and the lives of our patients matter in the kingdom of God. Faith is important in healthcare settings. Christian healthcare professionals have been given a great responsibility, as well as opportunity to be witnesses for Christ in the healthcare setting. Barriers exist, but tools can overcome them. Finally, we are not called to do this alone. In Acts 1:8, Jesus lets us know that we become his witnesses when we receive the Holy Spirit, who works in us and through us to this hurting world.
We can reach others by cultivating, sowing, and sometimes even harvesting right where we are in clinics and bedsides. We just need to open our own hearts to be used by the Holy Spirit. It is not us, but God who works through us and gives us the amazing opportunity to be a part of his kingdom work in the world.
The Saline Process is a program of IHS Global. It has been conducted in 126 countries (over 40 hostile/restricted) and in 43 language translations, through a partnership with global Christian healthcare organizations. Over 44,000 people have taken the Saline Process training since 2006 and are equipped as witnesses for Jesus in their healthcare settings. You can be, too. Contact us at saline@ihsglobal.org to get connected to a Saline Process training. You can also take a self-guided online training at ihsglobal.org/SPOT.

Latha Mathew, (lmathew@ihsglobal.org) serves with IHS Global. She and her husband, Mathew, are both dentists. In the 1990s, they pioneered rural dentistry while serving at a mission hospital in northern India. They went on to train others in their dentistry techniques and in missions. In 2021, she and Matthew moved to Kerela in the south of India where her involvement with the Saline Process continued. They have one daughter.

Lindsey Miller (lmiller@ihsglobal.org) serves IHS Global by supporting partners and volunteer trainers around the world. Lindsey studied international development, political science, and mathematics at Virginia Tech, and obtained a graduate degree in international development from Eastern University. Before joining IHS Global, she lived and worked in the rural mountains of Costa Rica in an area that had suffered a devastating earthquake. She lives in Utah with her husband and two small children.
[i] Harold G. Koenig, “Religion, Spirituality, and Health: The Research and Clinical Implications,” International Scholarly Research Notices, vol. 2012, accessed June 1, 2023, https://doi.org/10.5402/2012/278730.
[ii] Holly G. Atkinson, MD, David Fleenor, BCC, Susan M. Lerner, MD, Edward Poliandro, PhD, and Joseph Truglio, MD, MPH, “Teaching Third-Year Medical Students to Address Patients’ Spiritual Needs in the Surgery/Anesthesiology Clerkship,” MedEdPORTAL (2018), accessed June 1, 2023, https://doi.org/10.15766/mep_2374-8265.10784.
[iii] Gregory Makoul, “Contemporary issues in medicine: Communication in medicine,” in Report III: Contemporary issues in medicine: Communication in Medicine, Association of American Medical Colleges, medical school objectives project (Washington, DC: AAMC, 1999), accessed March 1, 2021.General Medical Council, “Personal Beliefs and Medical Practice,” accessed April 1, 2021, https://www.gmc-uk.org/ethical-guidance/ethical-guidance-for-doctors. International Council of Nurses, “International Council of Nurses (ICN) Code of Ethics for Nurses” (2021), accessed June 9, 2022, https://www.icn.ch/sites/default/files/2023-04/ICN_Code-of-Ethics_EN_Web_0_0.pdf. Diagnosis Review Committee, “New and Revised Diagnoses,” Nursing Diagnosis 13, no. 2 (2002): 68–71, Philadelphia: NANDA, accessed June 9, 2023, https://www.scribd.com/doc/298071128/Nursing-Care-Plan-for-Readiness-for-Enhanced-Spiritual-Well-Being-NCP. WHO Western Pacific, People-Centered Health Care: A Policy Framework, (Geneva, Switzerland: 2007), accessed September 15, 2021, https://www.who.int/publications/i/item/9789290613176.
[iv] Harold G. Koenig, “Religion, Spirituality, and Health: The Research and Clinical Implications,” ISRN Psychiatry, volume 2012 (December 16, 2012), accessed June 15, 2023, https://doi.org/10.5402/2012/278730.
[v] Kenneth I. Pargament, Harold G. Koenig, Nalini Tarakeshwar, and June Hahn, “Religious Struggle as a Predictor of Mortality Among Medically Ill Elderly Patients: A 2-Year Longitudinal Study,” Archives of Internal Medicine 161, no. 15 (August 27, 2001): 1881–1885, accessed June 15, 2023, https://pubmed.ncbi.nlm.nih.gov/11493130/.
[vi] George Fitchett, Patricia E. Murphy, Jo Kim, James L. Gibbons, Jacqueline R. Cameron, and Judy A. Davis, “Religious Struggle: Prevalence, Correlates and Mental Health Risks in Diabetic, Congestive Heart Failure, and Oncology Patients,” Int J Psychiatry Med 34, no. 2 (2004): 179–196, accessed June 15, 2023, https://doi.org/10.2190/ucj9-dp4m-9c0x-835m.
[vii] Jeanet Sinding Bentzen, “In Crisis, We Pray: Religiosity and the COVID-19 Pandemic,” Journal of Economic Behavior & Organization 192 (December 2021): 541–583, accessed June 15, 2023, https://doi.org/10.1016/j.jebo.2021.10.014.
[viii] “In Memorium: Francis Grim,” Frontline Missions South Africa, accessed June 1, 2023, https://www.frontlinemissionsa.org/in-memorium/francis-grim.
[ix] There are approximately 7.5 million Christian healthcare workers worldwide. This estimate is derived from the global count of Protestant Christians, which stands at 800 million (as reported by Pew Research in “Global Christianity: A Report on the Size and Distribution of the World’s Christian Population,” December 19, 2011, https://www.pewresearch.org/religion/2011/12/19/global-christianity-exec/), and the total number of global health workers, which is 65.1 million (as outlined in the publication by Boniol M, Kunjumen T, Nair TS, et al, “The Global Health Workforce Stock and Distribution in 2020 and 2030: A Threat to Equity and ‘Universal’ Health Coverage?” BMJ Global Health 7, no. 6 (June 2022): e009316, http://dx.doi.org/10.1136/bmjgh-2022-009316). It’s important to note that the estimate leans on a conservative approach regarding the count of Protestant Christians, as IHS Global collaborates with Catholic and Orthodox traditions in various regions. This number of Christian healthcare workers is likely conservative, especially considering countries like the US, where both Christian population and the number of healthcare workers are relatively higher.
[x] Our estimation assumes an average of 7,000 patient encounters per healthcare worker annually. This estimation is deliberately cautious due to substantial variations influenced by factors such as profession, specialization, and geographic location. For instance, the UK’s National Health Service (NHS) calculates different figures, indicating 2,260 patients per year for fully qualified GPs (excluding encounters, focusing solely on patients) and 3,700 patients annually for nurses (refer to the Office for National Statistics [ONS] release on December 9, 2022, available at the ONS website under the article “Trends in Patient-to-Staff Numbers at GP Practices in England: 2022,” https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/healthcaresystem/articles/trendsinpatienttostaffnumbersatgppracticesinengland/2022). Specifically, GPs in the UK handle an average of 41 patients each day (as reported by Denis Campbell, “One in 10 GPs See Twice as Many Patients as Safe Limit, Survey Finds,” The Guardian, May 7, 2019, https://www.theguardian.com/society/2019/may/08/gps-doctors-seeing-twice-as-many-patients-as-safe-limit-study). It’s notable that UK GPs allocate approximately 9 minutes per patient, whereas in the US, this duration extends beyond 20 minutes, and in India, it averages around 2 minutes (according to the systematic review by Irving G, Neves AL, Dambha-Miller H, et al, “International Variations in Primary Care Physician Consultation Time: A Systematic Review of 67 countries,” BMJ Open 7, no. 10 (2017): e017902, https://doi.org/10.1136/bmjopen-2017-017902).
[xi] Aaron Saguil and Karen Phelps, “The Spiritual Assessment,” American Family Physician 86, no. 6 (September 15, 2012): 546–550, accessed June 15, 2023, https://www.aafp.org/pubs/afp/issues/2012/0915/p546.html.
EMQ, Volume 59, Issue 4. Copyright © 2023 by Missio Nexus. All rights reserved. Not to be reproduced or copied in any form without written permission from Missio Nexus. Email: EMQ@MissioNexus.org.




