EMQ » July–September 2023 » Volume 59 Issue 4
[mepr-show rules=”100329″] [/mepr-show]
Summary: Ralph Winter describes four stages of development in mission/church relations: pioneer, parent, partner, and finally, participant. These stages can also be applied to mission hospitals particularly as they relate to the roles of expatriate and national medical missionaries. Analyzing these stages can help us discover where mission hospital development is stuck, and how to progress forward.
By Richard Davis, Evelyn Mbugua, Peter Halestrap, Ken Muma, Faith Lelei, and Chege Macharia
Several years ago, a surgeon at our hospital spent time with his mentor’s mentor – a surgeon who was at our hospital in the 1950s and 60s. The old surgeon fondly recalled an operating theater upgrade and the fine tile work he did as part of the upgrade. He was clearly proud of his work and how well it stood the test of time. He asked if the tile was still there? The younger surgeon told him he had no idea.
Currently, our hospital has 13 operating rooms. Neurosurgeons perform skull base and brainstem surgery. Head and neck surgeons perform reconstructive surgeries (known as microvascular free flaps). Orthopedic surgeons implant the same hardware you would receive in London or Los Angeles. Some of these surgeons are Africans and some are expatriate. Not one of us would ever think it was our job to lay tile if it was needed in the operating theatre.
Mission hospitals, their staff, and the roles staff play change over time. There is a normal, natural progression. But what steps does this progression entail, and what should the result be? Mission literature provides parallels we can explore.
Stages of Mission Development
In the Perspectives on the World Christian Movement: A Reader book (perspectives.org), Ralph Winter describes four stages of development in mission/church relations. During these stages, the expatriate missionary progresses through the following roles: pioneer, parent, partner, and finally, participant.
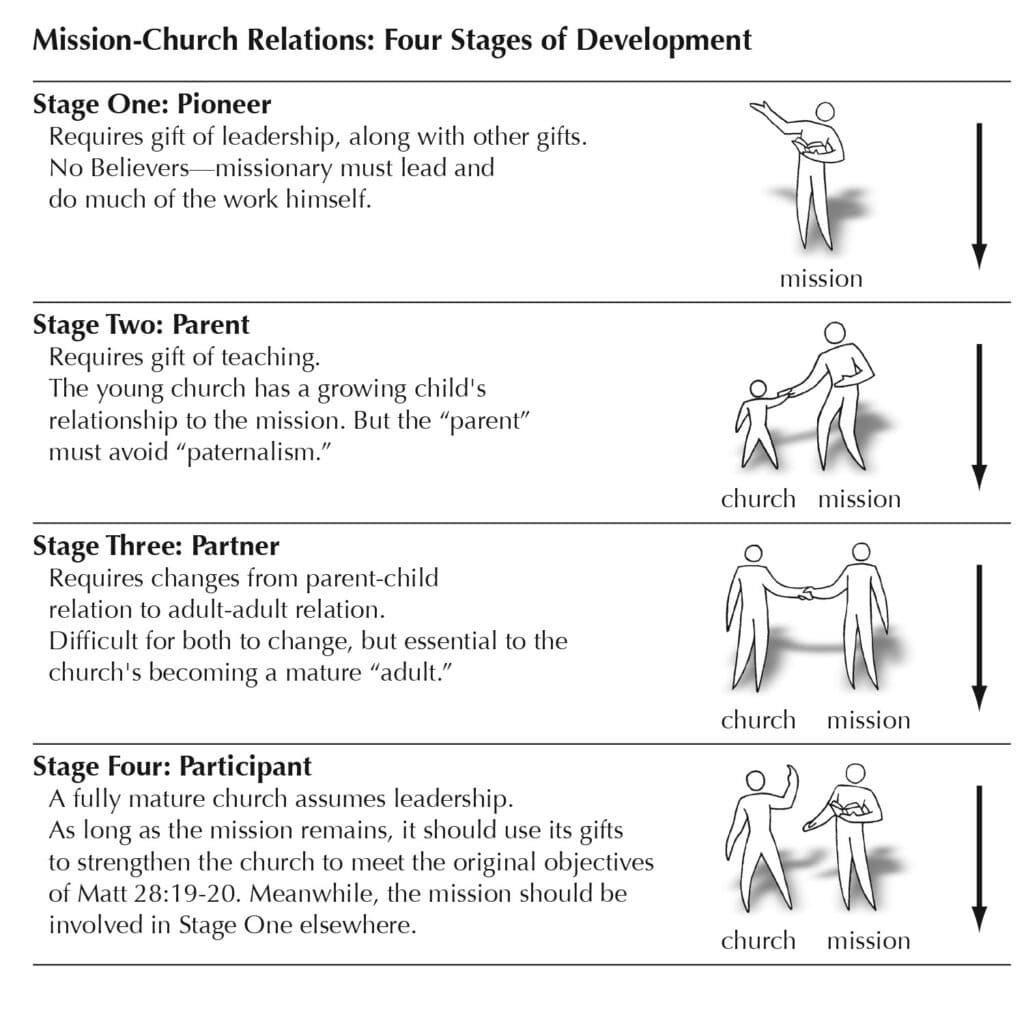
Caption: Figure 5.1 –Ralph Winter described four stages of development in mission/church relations as shown in this illustration.
These stages to the relationship can be extrapolated between the expatriate medical missionary and the hospital where they serve. The pioneer missionary is the founder of the hospital. This multitalented individual takes out the tumor, delivers the baby, rebuilds the diesel generator, designs, oversees construction of the hospital, and preaches every Sunday at the local church. This is what most people think of when they picture a medical missionary. When there is a problem, the pioneer is the one tasked with solving it.
As the hospital progresses, others do more tasks and solve more problems. The expatriate missionary moves into the next role. The parentis the boss, involved in every decision and on every committee. He or she controls the purse strings. Although the hospital may have a little revenue from patient care, any development or expansion will be through donors who can be accessed only through him.
There may be teaching of others, and delegation of tasks like rebuilding the diesel generator or laying tile. In fact, the hospital could not grow if there wasn’t such delegation. But the expatriate missionary is still the chief executive officer in every sense (even if someone else in the hospital holds that title!)
Many mission hospitals don’t progress beyond this stage, but if they can, the expatriate missionary becomes a partner. When this is the case, national people assume decision-making leadership roles. Perhaps these skilled workers trained at that hospital, or elsewhere. They gradually assume roles like chief finance officer, chief executive officer, medical director, department head. Each of these positions gets handed over from an expatriate to a national person, as qualified individuals arrive.
The number of national clinicians also increases, often drawn from among graduated trainees. Mentorship happens naturally in training programs, producing competent clinicians who share the kingdom-minded worldview of their teachers. Eventually they can take over clinical care and training programs as well. Since these workers are part of the mission of the hospital, they are rightly called national, or indigenous missionaries.
In the final stage, the expatriate missionary is now a member of the team – a participant. This individual doesn’t have the best house on the mission station. He or she isn’t on the board. This person’s supervisor is national, and this supervisor is free to give orders, critically evaluate performance, or even terminate employment. The expatriate missionary is a respected adviser, but his or her advice isn’t automatically followed.
Transitioning from Parent to Partner
We believe that the most difficult transition in these stages may be from the second to the third stage, from parent to partner. There are many reasons why this transition can be difficult. Letting go can be challenging. Just as real parents can struggle to release their children and see them make decisions or life choices they may not personally like, so missionary parents can thus inappropriately try to retain control. They may also struggle with losing their voice on decisions and often associated privileges of being in senior positions, such as housing, and work schedules.
The transition can be seen to occur too quickly for certain people, with concerns about corruption, political or church interference, and loss of donor money as the expatriate missionaries scale back. Surprisingly, nationals – both inside and outside the hospital – are sometimes the biggest opponents to expatriate missionaries stepping out of leadership roles.
Conversely the transition can feel too slow for other people. This can result in national staff that do not see opportunities to utilize their skills to grow and develop the institution leaving. The best houses, positions, and leadership opportunities still seem to be reserved for expatriates. Talk about “developing leadership” can seem like mere lip service.
It may be difficult to find individuals with the right academic qualifications and experience within the country. Appropriate national missionaries to take on the leadership of the hospital may be lacking.
However, even when these individuals are plentiful it can be challenging for the hospital to provide remunerationpackages that recruit and retain the required talent. This cost will often need to be passed onto patients. This risks mission drift away from caring for the most vulnerable.
Given these potential challenges, we have several observations on what conditions will help a hospital reach the stage where expatriate missionaries can become partners, and then participants.
1. Train Well
A commitment to training and empowering indigenous workers is mandatory. A graduate medical education program (such as a medical or surgical residency) can be difficult to set up. Obtaining recognition by the country’s medical board can be time-consuming and difficult. But it is worth it. Training is the best possible source of future national missionaries. Those who stay understand the hospital’s vision and share its values. And the hospital has the advantage of knowing these future leaders very well, as they have completed a 3- to 5-year job interview during training.
Trainees in a mission hospital should get more than tangible procedural skills, clinical judgment and training, or managerial competencies. Mentorship speaks into what it means to be a Christ-like physician: work ethic, humility, and ethics of care, especially care for the poor and vulnerable. Modeling this behavior helps trainees experience and inherit non-tangible qualities – that group of shared values and behaviors that we call culture.
The culture of a mission hospital is especially important given its base in its values, its literal mission. When national partners share that culture and want to see it protected, the hospital will be healthy in their hands as the expatriate missionary’s role changes to partner or participant. The focus quite naturally becomes the shared vision and resulting work of a team, rather than of one individual.
Our hospital recently completed a search for a new chief executive officer. After two rounds in an international search, the committee had reviewed many qualified master’s and PhD candidates with extensive leadership experience, but hadn’t yet found the right fit.
Finally, for the third cycle, they expanded the search to candidates with a professional graduate degree alone, which allowed several internal candidates to be considered. The one chosen was a graduate of one of the hospital’s own residency programs. the hospital board unanimously agreed that this was the candidate they had been looking for all along.
If a hospital has a reputation for excellence in training, it will be able to choose from the best of the applicants, mentor them well, and then choose the best of these to remain at the hospital. In this way, high-quality training naturally increases the overall quality of a hospital, bringing in the most suitable indigenous partners to continue its vision.
Our hospital is enjoying the fruits of this process: our graduates have filled positions at our hospital including as two of the last three executive directors, the two most recent clinical directors, and almost all of the current program directors of our training programs.
2. Recognize Shared Mission and Vision
Expatriate missionaries and national partners have a shared mission and vision of serving God. Both are truly missionaries, and both should regard each other as such. Even in the developing world, well-paying jobs for well-trained physicians are available, serving the wealthy in the large cities. The graduates of our hospital would be well-positioned to take these jobs.
However, by choosing to stay with us instead, they choose a more humble and less lucrative path. Often, they must resist pressure from family members (some of whom paid their tuition) to make as much money as possible. It is important for the expatriate missionaries to recognize that their national colleagues are also missionaries, having also made tremendous sacrifices to serve.
A national physician leader tells us, “When you (expatriates) go to your home church, the people say ‘You are doing such good work. Let me give you some money.’ But when we go to our home church, the people say ‘You are doing such good work. Give me some money.’”
3. Remember We Are All Sinners
It is important to see everyone we work with as someone made in God’s image, loved by him and whom Jesus died for. Equally we need to remember we are all sinners saved by grace that sometimes make mistakes. Understand that most of the misunderstandings we face on the mission field are cultural in nature, for all parties.
Both national and expatriate workers must assume the best when faced with difficult situations. This can be especially tricky in times of stress, when your barriers are down. Unfortunately, such stressful times are all too common in healthcare. Be willing to forgive each other easily. Be joyful in hope, patient in affliction, faithful in prayer (Romans 12:12). The best way to overcome cultural stress is through deliberate prayer about it, at the individual and corporate level.
The traits that make a missionary succeed at the pioneer and parent phases are independence, stubbornness, and even the ability to ignore sensible advice. But at the partner and participant phases, these traits are liabilities. In the business world, this is called founder’s syndrome.[i]
And just like in business, sometimes pioneers need to get out of the way if the hospital is to progress. These transitions can be painful and cause resentment among both expatriates and national staff. They can also lead to loss of the donor funds because of the purse strings that the expatriate missionary held.
4. Develop a Written Strategy
We believe well formulated, agreed to, and written strategy is required. What goals were the founding missionaries trying to achieve? Did they want their hospital to stay the way it always had been (with them in charge?) Or did they want it to progress to a viable, independent institution? Does everyone agree with this goal, and is there a plan to make this happen? Does the country’s economy and state of development as a whole make this possible?
These questions are best answered by the hospital’s vision, mission, and values statements and a strategic plan. Without a long-term goal, a hospital will not survive the inevitable departure of its founders and the changing environmental circumstances. As an institution we have found these documents essential to keep the focus and vision of the hospital.
In 2017 our hospital went through a leadership crisis and new management was put in place by the board. The new senior management team was led by one of our residency graduates. This team, predominantly national, revived the mission and vision of the hospital and wrote a new strategic plan. Over the last six years there have been several changes in the senior management team of the hospital, including four clinical directors (two expatriate and two national). Despite these changes, the strategic plan was followed and the majority its goals achieved.
One constant request from the leadership was that the expatriate missionaries would always have a representative on the senior management team, to help the hospital maintain its original values. This individual’s role could truly be described as partner. Their presence served as a reminder of what the founders of the hospital had conceived. The nationals want the expatriates to stay around, often as more than participant.
Ensuring Longevity
Hospitals aren’t the same as churches, so perhaps this analogy breaks down at some point. As our hospital continues to serve a poor population in a developing country, we benefit from intellectual exchange with clinicians from more developed locations. So it helps when the partners/participants remain.
Sometimes we can leapfrog certain steps that would be required to develop a complex program. Reconstructive and joint surgeries as well as critical care for adults, children and infants are all examples where pioneers became partners and continue to walk with us as participants. These little progressions continue to happen wherever there is a perceived need for a new clinical or educational service.
We also benefit strongly from an organized fundraising process, whereby individuals in developed nations can be partners as well, agreeing with the work that is being continued by nationals and expatriates together. This process is also a team effort, rather than the work of one pioneer individual. It is naturally stronger and more effective than the fundraising work of one individual ever could be. Where does your favorite mission hospital sit on the Pioneer → Parent → Partner → Participant scale? If it is stuck at one level, are the obstacles external or internal? Is there willingness among the missionaries to move along this scale? Is there willingness among the national people? Recognizing where we are stuck is the first step towards progressing through these development stages and ensuring the longevity of our shared strategic mandate.
Richard Davis, MD, (rich.davis.paacs@gmail.com) is a general surgeon and former director of clinical services at AIC Kijabe Hospital.

Evelyn Mbugua, MD,(evelynmbugua@gmail.com) is an internal medicine physician, former director of clinical services at AIC Kijabe Hospital, and current executive director of AIC CURE Hospital Kijabe.

Peter Halestrap, MD,(direduc@Kijabehospital.org) is a family medicine physician, former director general, and current director of graduate medical education at AIC Kijabe Hospital.

Ken Muma, MD,(HeadPaedSurg@kijabehospital.org) is a graduate of the pediatric surgery residency, program director of the pediatric surgery residency, and former director general at AIC Kijabe Hospital.

Faith Lelei, MD,(dirclin@kijabehospital.org) is a graduate of the Family Medicine residency, a family medicine physician, and current director of clinical services at AIC Kijabe Hospital.

Chege Macharia, MD,(execdir@kijabehospital.org) is a graduate of the general surgery residency, a general and head and neck surgeon, and current director general at AIC Kijabe Hospital
[i] Katie Koenig, “What Is Nonprofit Founder’s Syndrome?” 501(c)(3) Business Services, April 5, 2021, https://www.501c3.org/what-is-nonprofit-founders-syndrome/.
EMQ, Volume 59, Issue 4. Copyright © 2023 by Missio Nexus. All rights reserved. Not to be reproduced or copied in any form without written permission from Missio Nexus. Email: EMQ@MissioNexus.org.




